DBP3:Utah:RegSegPipeline
From NAMIC Wiki
Revision as of 14:30, 11 February 2011 by Meier (talk | contribs) (→Pilot Studies on a Registration & Segmentation Pipeline & Workflow)
Home < DBP3:Utah:RegSegPipeline
back to DBP3 home
The CARMA DBP: MRI-based study and treatment of atrial fibrillation
Alex Zaitsev, Dominik Meier, Ron Kikinis
Pilot Studies on a Registration & Segmentation Pipeline & Workflow
Overall processing steps are (order tentative)
- N4 bias field correction for the MRI (surface coils):
- run on entire image gives some benefit that may be improved with masking: again the dominant intensity dropoff from the surface coil occurs along the chest wall and ribcage. Even if that is not the structure of interest, it is the low-freq. variation the bias correction algorithm is searching for, and masking that out can be counter-productive: via masking we may end up with a smoother image, but the intensity variations removed were not caused by the coil but are actually true signal.
- Module used: N4 ITK
- registration MRA>cMRI
- the MRA contains the same FOV and has surrounding structures (liver, chest, spine etc) visible also, despite lower intensities. A global affine is thus not necessarily going to benefit from masking the heart, unless the relative motion of the heart becomes the dominant reason for misalignment.
- Module used: BRAINSfit
- ROI definition (manual box ROI or automated via atlas)
- segmentation of LA from MRA -> inner wall
- as a dynamic image the MRA contains significant spread and likely requires interactive segmentation/thresholding to yield a satisfactory LA volume
- Module used: Editor: thresholding or thresholding within Volumes thresholding option within Display tab, use iron colormap & low alpha setting to check for ventricular wall borders.
- cropping and island removal
- LA wall segmentation
- very small structure, most reliably done manually direct. Starting with automation may yield more effort on post-edits
- Module used: Editor: manual outline
- segmentation of enhancement within LA wall: intensity statistics. An atlas-based set of intensity distributions may be more meaningful here than a simple Otsu, because both amount and location of enhancement is unknown and can in theory be 0.
- registration follow-up -> baseline
- most reliably done on the post contrast MRI.
- DOF of 12 or even low-res BSpline should be ok
- Module used: BRAINSfit

Example contrast MRI with thresholded MRA as color overlay. Registration validation is not trivial: we can in theory use the position of the blood in the MRA relative to the LV wall as registration check, but the MRA itself does not provide a clear boundary at the lower intensities.

Example contrast MRI with thresholded MRA as color overlay and areas of enhancement marked
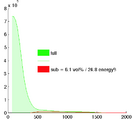
Histogram of MRA intensities: green = entire FOV, red: cardiac structures only (excl. aorta), which make only 6% of the total image content and thus are unlikely to disturb a registration based on the entire image.


