DBP3:Utah:RegSegPipeline
back to DBP3 home
Contents
The CARMA DBP: MRI-based study and treatment of atrial fibrillation
Alex Zaitsev, Dominik Meier, Ron Kikinis
Pilot Studies on a Registration & Segmentation Pipeline & Workflow
Main processing pipeline
- N4 bias field correction for the MRI (surface coils):
- run on entire image gives some benefit that may be improved with masking: again the dominant intensity dropoff from the surface coil occurs along the chest wall and ribcage. Even if that is not the structure of interest, it is the low-freq. variation the bias correction algorithm is searching for, and masking that out can be counter-productive: via masking we may end up with a smoother image, but the intensity variations removed were not caused by the coil but are actually true signal.
- Module used: N4 ITK; Parameters: convergence: 1e-5, iterations: 50,40,30,20, shrink factor: 3
- registration MRA>cMRI
- the MRA contains the same FOV and has surrounding structures (liver, chest, spine etc) visible also, despite lower intensities. A global affine is thus not necessarily going to benefit from masking the heart, unless the relative motion of the heart becomes the dominant reason for misalignment.
- Module used: BRAINSfit
- tried masking with both BrainsFit and RobustMultires modules. Both failed to provide better alignment with masking.
- images have good alignment to begin with, need reliable fiducial to evaluate registration. E..g. descending aorta? non-cardiac structures?
- registration follow-up -> baseline
- most reliably done on the post contrast MRI.
- DOF at least 12, because image is captured at different phases in the breathing/cardiac cycle, some low-res BSpline should be beneficial
- Module used: BRAINSfit
- the IS FOV can differ, e.g. how much of the liver is included. If the two exams differ significantly (>30%) in that content, a prior cropping step is suggested to better match image content before registration. Resampling to isotropic voxel size at this stage is also advantageous.
- ROI definition (manual box ROI or automated via atlas)
- segmentation of LA from MRA -> inner wall
- as a dynamic image the MRA contains significant spread and likely requires interactive segmentation/thresholding to yield a satisfactory LA volume
- Module used: Editor: thresholding or thresholding within Volumes thresholding option within Display tab, use iron colormap & low alpha setting to check for ventricular wall borders.
- cropping and island removal
- LA wall segmentation
- very small structure, most reliably done manually direct. Starting with automation may yield more effort on post-edits
- Module used: Editor: manual outline
- segmentation of enhancement within LA wall: intensity statistics. An atlas-based set of intensity distributions may be more meaningful here than a simple Otsu, because both amount and location of enhancement is unknown and can in theory be 0.

Example contrast MRI with thresholded MRA as color overlay. Registration validation is not trivial: we can in theory use the position of the blood in the MRA relative to the LV wall as registration check, but the MRA itself does not provide a clear boundary at the lower intensities.

Example contrast MRI with thresholded MRA as color overlay and areas of enhancement marked
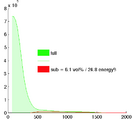
Histogram of MRA intensities: green = entire FOV, red: cardiac structures only (excl. aorta), which make only 6% of the total image content and thus are unlikely to disturb a registration based on the entire image.

Bias field correction results (N4ITK) with and without masking of the structures of interest. Masking causes a different correction not related to coil sensitivity but rather local image content. Masking is not recommended at this point.




Example Cases
- Example Case P2 : pre-post registration
- This example contains significant MRI (motion?) artifacts that require dedicated processing to isolate the structures of interest
- E.g. FOV includes much more of liver on pre exam, which needs to be cropped to amount matching the follow-up