Difference between revisions of "2013 Winter Project Week Gyne Brachy"
From NAMIC Wiki
| Line 27: | Line 27: | ||
<div style="width: 27%; float: left; padding-right: 3%;"> | <div style="width: 27%; float: left; padding-right: 3%;"> | ||
<h3>Progress</h3> | <h3>Progress</h3> | ||
| − | * | + | * To compare the segmented needles from MRI and CT, we tried different landmarks to for registration and we conclude that the best rigid anatomical landmark for this purpose is the hip bone. |
| + | * We found out that the needles displaced noticeably and their shapes has been changed by the patients position change from partial lithotomy position (the MRI data) to supine position (the CT data). This implies that in order to be able to use the CT data for validation iGyne needle segmentation tool, we need to modify our workflow and add a supine position MRI to our IGT Gyne workflow. | ||
| + | * Our findings about the needle position and shape changes demands a further investigation to understand and model those changes and their possible effect on the treatment results. | ||
| + | * For the purpose of needle segmentation results validation we will add 3D point correspondence and similarity measures to iGyne module soon. | ||
</div> | </div> | ||
</div> | </div> | ||
Revision as of 08:08, 11 January 2013
Home < 2013 Winter Project Week Gyne Brachy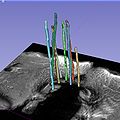
Segmented Brachytherapy Needles in iGyne.


Key Investigators
- Alireza Mehrtash, Tina Kapur, Guillaume Pernelle, Jan Egger, Neha Agrawal, Antonio Damato, BWH
- Csaba Pinter, Queen's
Project Description
Objective
- The iGyne module is a user friendly Slicer module which is designed to assist gynecologic radiation oncologists in the process of applicator placement and brachytherapy needle insertion. Currently the module can perform applicator registration and needle segmentation successfully.
- The objective of this project is to develop a method to validate and measure the accuracy of the needle segmentation results.
Approach, Plan
- Needle digitization.
- Exporting the segmented needles.
- Make a comparison between the segmented needles from MRI images and the postoperative checking CT images.
- Define metrics to measure the accuracy of the segmentation results.
Progress
- To compare the segmented needles from MRI and CT, we tried different landmarks to for registration and we conclude that the best rigid anatomical landmark for this purpose is the hip bone.
- We found out that the needles displaced noticeably and their shapes has been changed by the patients position change from partial lithotomy position (the MRI data) to supine position (the CT data). This implies that in order to be able to use the CT data for validation iGyne needle segmentation tool, we need to modify our workflow and add a supine position MRI to our IGT Gyne workflow.
- Our findings about the needle position and shape changes demands a further investigation to understand and model those changes and their possible effect on the treatment results.
- For the purpose of needle segmentation results validation we will add 3D point correspondence and similarity measures to iGyne module soon.